

Case Study
Conducted by Christopher Sanders, M.D.
March 8, 2023
HPI: 70 y/o WM with Stage 3 decubiti left and right buttocks sent to the rehabilitation from the hospital s/p CVA. Patient was wheelchair bound at home and sent to hospital for a recurrent CVA. Wounds were present at home. Unknown stage and Rx.
PMHx: Type 2 diabetes mellitus, well controlled, nicotine dependence, COPD, Congestive Heart Failure, cerebrovascular accident, Left hemiplegia, GERD, Tachycardia, Covid 19, Hyperlipidemia, Hypertension, and Heart disease, with a weight: 235 lbs.
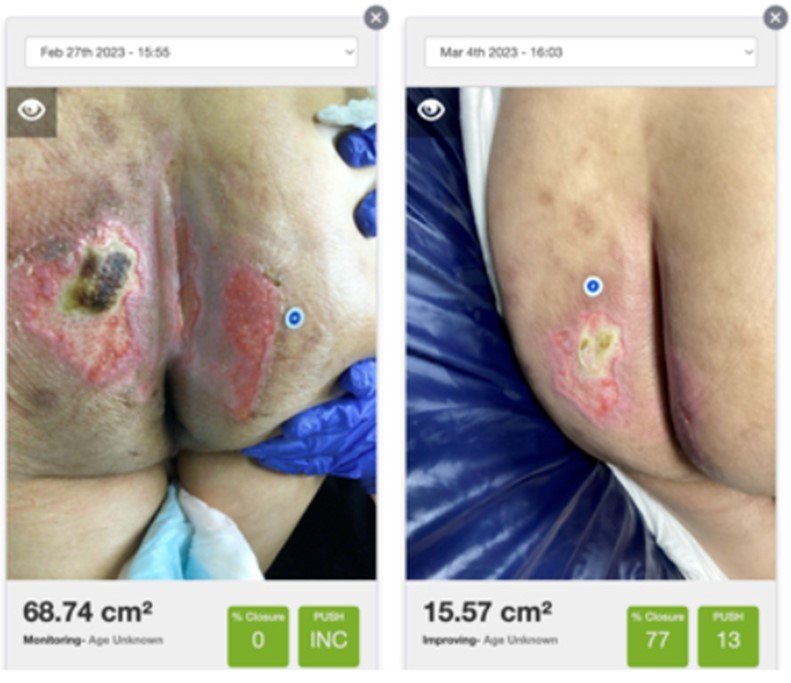
Wound: As is evident in the picture, the wound on left picture is a stage 3 decubiti. The wound on left buttock is composed of eschar, slough, and small patches of granulation. The lateral wound margin is ill defined. The linear, vertical wound on right buttock is majority slough with scattered granulation and well-defined margins. The most lateral wound on right buttock is a stage 2 majority granulation tissue.
I saw the wound in the early evening of Day 1, and signed input orders which were executed that evening. The orders were to mechanically debride/wash all the wounds using DSG saturated with Spectricept™ prior to application of dressing. Spectricept™ is a 510(k) cleared wound cleanser product. The nurse then applied Santyl to all eschared areas, Mesalt sodium chloride to sloughed/any other open areas, and Aquaphor to any remaining areas. She then covered the wounds with dry gauze, cover entire area with ABD, and secured. the dressing. We used a rolling protocol. Perform QD. The order was executed that evening and daily thereafter per physicians’ discretion, until dry sterile gauze (DSG) was removed on Day 6, when the second picture was taken. A wound like this would normally take at least a month to heal with fastidious care, but there are numerous variables that are somewhat unpredictable.
Solutions such as Spectricept™ are used to aid in mechanical removal of debris from the wound bed. Polymicrobial organisms are released into the wound bed by the dissolution of eschar/slough by the collaganase/fibrinolytic dressing. The currently available wound solutions for use are non-sterile OTC commercial wound cleansers and some product with lower HOCl dosages. Spectricept is approved as a multi-use prescription product and it is highly antimicrobial in solution with a powerful preservative effect allowing for the reuse of the same bottle.
Clinicians are re-dressing a contaminated wound every time, constantly culturing, and treating with antibiotic gels which are relatively ineffective. In my opinion, this is why these wounds take so long to heal as they are not being properly debrided and cleaned and the constant discharge which contains polymicrobial load can further contaminate surrounding lesions. This is why there is a requirement for multiple dressings on the wounds, extended staff time for application, and more dressing materials to cover wounds, which always cost more time and money. Most often the actual treatment is being done by a nurse or an LPN not necessarily trained in wound care. Often, the patient is treated by many different nurses, so there may not be a consistency in the treatment protocol regimen. The use of Spectricept™, may help close some of the gaps or potential deficiencies in wound management.
Debridement and cleaning with Spectricept™ prior to DSG application may be proven to properly remove contamination and unwanted debris from the wound bed.. The cleaning and removal of wound biofilms and other bioburdens will be the subject for future peer reviewed clinical studies planned to be initiated by independent practicians.
As impressive as the healing action on the left buttock is, I am more impressed with the sloughed out, longer wound just to the right of the gluteal crease. It is healed but for a tiny spot towards the bottom of the wound. It is fully epithelialized and completely healed in six days. I have never seen this happen so quickly in 14 years of wound care clinical practice. I have no clinical explanation for the rapid healing of the left buttock, and the complete healing on the right except for the use of Spectricept but to assume excellent debridement without removing deeper layers of tissue. It is the only thing that I did different from our normal wound care protocol. Deductive reasoning leads to one inevitable conclusion, Spectricept made the difference in the outcome. From this point forward, for future patients, we will revise all future orders to use the Santyl with Spectricept™.
Christopher Sanders, M.D.
Independent physician Investigator