The Biofilm Challenge : Why Traditional Antimicrobials Fail in Chronic Wounds
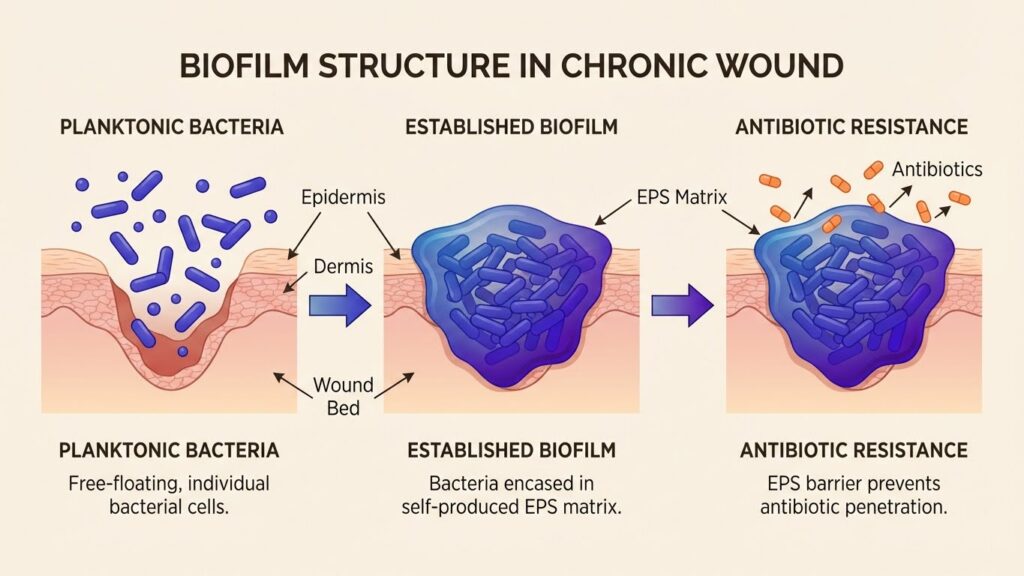
Imagine a wound that refuses to heal despite months of treatment. The patient receives antibiotics, undergoes regular dressing changes, and follows all medical advice—yet the wound persists, trapped in a cycle of inflammation and infection. This frustrating scenario affects millions of patients worldwide, and science now understands why: biofilms. Recent research estimates that biofilms are present in almost all chronic wounds, with studies reporting prevalence rates between 60% and 100% in non-healing wounds. These microscopic communities of bacteria create a nearly impenetrable fortress that renders conventional antimicrobial treatments largely ineffective. According to a 2025 study published in Biomedical Journal, global healthcare costs associated with biofilm-induced chronic infections are estimated at approximately $386 billion annually. For healthcare professionals treating chronic wounds—whether diabetic foot ulcers, pressure injuries, or surgical site infections—understanding biofilms is no longer optional. It’s essential. What Are Biofilms? Understanding the Architecture Biofilms are structured communities of bacterial cells that adhere to surfaces and encase themselves in a self-produced extracellular polymeric substance (EPS). Think of them as bacterial cities, complete with infrastructure, communication systems, and sophisticated defense mechanisms. The EPS matrix consists of: This complex architecture creates multiple layers of protection. The outer layers of bacteria may be metabolically active, while those deep within enter a dormant “persister” state that makes them extraordinarily resistant to antimicrobial agents. The Biofilm Formation Process Biofilm development follows a predictable sequence: Stage 1: Initial Attachment Planktonic (free-floating) bacteria encounter a wound surface and begin adhering through weak, reversible bonds. This stage typically occurs within minutes to hours. Stage 2: Irreversible Attachment Bacteria strengthen their attachment through specific adhesins and begin producing EPS components. This transition marks the point where simple cleansing becomes insufficient. Stage 3: Maturation The bacterial community grows and differentiates. Microcolonies form, and the EPS matrix thickens. Channels develop within the biofilm, allowing nutrient distribution and waste removal. Stage 4: Dispersion Bacterial cells detach from the mature biofilm and colonize new areas. This stage explains why biofilms can spread rapidly within wounds and why recurrence is so common. Why Traditional Antibiotics Fail Against Biofilms The therapeutic failure of conventional antimicrobials against biofilm-associated wound infections stems from multiple mechanisms: 1. Physical Barrier Protection The EPS matrix acts as a molecular sieve, slowing antibiotic penetration. By the time antimicrobial agents reach bacteria in the biofilm’s deeper layers, concentrations may be 100-1,000 times lower than necessary for bacterial killing. 2. Altered Microenvironment The biofilm interior creates unique conditions—low oxygen tension, acidic pH, and nutrient limitation—that fundamentally alter bacterial metabolism. Many antibiotics target actively growing bacteria, making them ineffective against slow-growing or dormant biofilm cells. 3. Persister Cells These are phenotypic variants that enter a dormant state, making them inherently tolerant to antibiotics. Research shows that persisters can represent 1-10% of biofilm populations. They survive antibiotic treatment and repopulate the biofilm once treatment ceases. 4. Increased Genetic Exchange The close proximity of bacterial cells within biofilms facilitates horizontal gene transfer, including antibiotic resistance genes. This creates hotspots for the evolution and spread of antimicrobial resistance. 5. Quorum Sensing Communication Bacteria within biofilms use chemical signaling molecules to coordinate behavior, including upregulation of resistance genes and production of enzymes that inactivate antibiotics. The Clinical Impact: Why Biofilms Matter The presence of biofilms fundamentally changes wound healing dynamics: A 2025 consensus document from the World Union of Wound Healing Societies now states that “all non-healing chronic wounds potentially harbor biofilms” and recommends that treatment should target biofilm disruption and prevention of reformation. Current Approaches to Biofilm Management The medical community has developed a multi-faceted strategy known as Biofilm-Based Wound Care (BBWC): Aggressive Debridement Mechanical removal of biofilm through sharp debridement, ultrasonic methods, or enzymatic approaches. This temporarily reduces bacterial burden and makes remaining bacteria more susceptible to antimicrobials. Cleansing and Irrigation Use of wound cleansers to physically remove planktonic bacteria and debris. However, standard irrigation alone cannot eliminate established biofilms. Antimicrobial Dressings Application of silver, iodine, or other antimicrobial-containing dressings. These can help suppress biofilm reformation but often cannot penetrate established biofilms. The “Step-Down Approach” This strategy involves repeated debridement followed immediately by antimicrobial application, with treatment intensity adjusted based on healing progress. The Challenge Remains: Need for Innovation Despite these interventions, biofilm management remains frustratingly difficult. Current approaches face several limitations: The Promise of Next-Generation Solutions The biofilm challenge has driven innovation in antimicrobial development. Researchers are pursuing several promising approaches: 1. Biofilm-Penetrating Agents New antimicrobials designed to disrupt or penetrate the EPS matrix, reaching bacteria that conventional agents cannot touch. 2. Anti-Biofilm Enzymes Enzymes that specifically target components of the EPS matrix, breaking down the protective structure. 3. Quorum Sensing Inhibitors Molecules that disrupt bacterial communication, preventing coordinated biofilm formation and maintenance. 4. Combination Therapies Synergistic approaches that combine physical disruption with multiple antimicrobial mechanisms. 5. Advanced HOCl-Based Solutions Next-generation hypochlorous acid formulations that maintain efficacy in the presence of organic matter—a critical limitation that has prevented traditional HOCl products from addressing biofilms effectively. Looking Forward: A New Era in Wound Care The biofilm challenge represents one of the most significant obstacles in modern wound care. As our understanding of these bacterial communities deepens, so does our ability to develop targeted interventions. Recent advances in antimicrobial chemistry, particularly formulations that maintain stability and efficacy in challenging wound environments, offer hope for improved outcomes. The key lies in solutions that can: For healthcare providers on the front lines of wound care, staying informed about biofilm biology and emerging treatment strategies is essential. The patients whose wounds refuse to heal deserve access to innovations that finally break through the biofilm barrier. Conclusion Biofilms represent a formidable challenge in chronic wound management, but they are not insurmountable. Through continued research, clinical innovation, and the development of next-generation antimicrobials specifically designed to overcome biofilm protection mechanisms, we are entering a new era in wound care. The goal is clear: transform chronic, non-healing wounds into acute, healing wounds by effectively managing the biofilm communities that perpetuate infection and inflammation. With the right tools and approaches, this goal is increasingly within
Beyond Antibiotics : How HOCl-Based Solutions Combat Antimicrobial Resistance
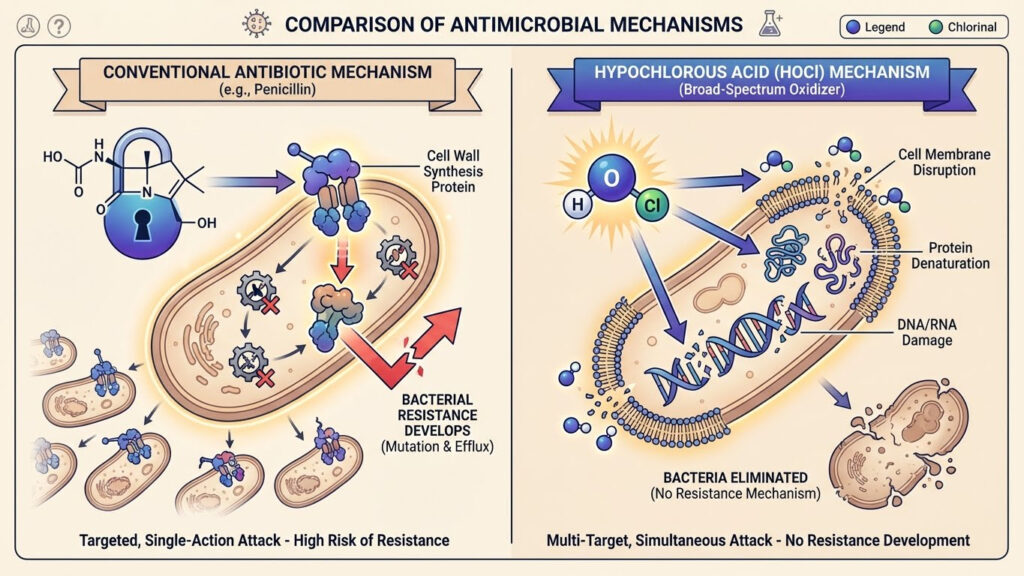
Beyond Antibiotics : How HOCl-Based Solutions Combat Antimicrobial Resistance The Growing Crisis: When Antibiotics Stop Working In 2025, antimicrobial resistance (AMR) has emerged as one of the most pressing threats to global health. The World Health Organization warns that drug-resistant infections could claim more lives than cancer by 2050 if current trends continue. Every time a doctor prescribes antibiotics, every time a patient fails to complete their antibiotic course, every time antibiotics are used unnecessarily, resistant bacteria gain an evolutionary advantage. The statistics are sobering: Infections caused by antimicrobial-resistant pathogens now contribute to approximately 1.27 million deaths globally each year. Methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE), and multi-drug resistant Pseudomonas aeruginosa are no longer hospital curiosities—they’re everyday challenges in clinical practice. But what if there was an antimicrobial agent that bacteria have been exposed to for millions of years yet have never developed meaningful resistance against? Enter hypochlorous acid (HOCl), a molecule your own immune system produces to fight infections. HOCl: Nature’s Original Antimicrobial Hypochlorous acid isn’t a laboratory invention—it’s biology’s answer to microbial threats. When your body detects an infection, neutrophils (white blood cells) rush to the site and produce HOCl through an enzyme called myeloperoxidase. In fact, approximately 70% of hydrogen peroxide produced by neutrophils is converted into HOCl. This powerful oxidant is your immune system’s first line of defense against invading pathogens. Consider this remarkable fact: An estimated 10⁶ stimulated neutrophils can produce approximately 0.2 μmol of HOCl during a 2-hour period. That tiny amount is enough to destroy 150 million E. coli cells in milliseconds. This extraordinary potency, combined with its rapid action and natural occurrence in the body, makes HOCl fundamentally different from synthetic antibiotics. How HOCl Works: A Multi-Target Approach Unlike antibiotics, which typically target specific bacterial structures or processes (like cell wall synthesis or protein production), HOCl operates through a multi-faceted mechanism that makes resistance development extraordinarily difficult. Multiple Cellular Targets HOCl interacts with several biomolecules simultaneously: This multi-pronged attack means bacteria would need to simultaneously develop multiple resistance mechanisms—a virtually impossible evolutionary feat. As one researcher noted, it would be like trying to defend a castle when attackers are breaching the walls, the gates, the moat, and tunneling from below all at once. The Speed Advantage HOCl’s antimicrobial action occurs within seconds. Recent studies demonstrate that stabilized HOCl solutions kill bacteria within the first minute of contact, with accurate killing times as short as 12 seconds. This rapid action prevents bacteria from activating stress response mechanisms or initiating resistance gene expression. The Resistance Question: Why HOCl Succeeds Where Antibiotics Fail The fundamental difference between HOCl and conventional antibiotics lies in their mechanisms of action and bacteria’s ability to adapt. Antibiotic Resistance Mechanisms Bacteria develop antibiotic resistance through several well-characterized mechanisms: HOCl Resistance: Theoretical But Rare While research has identified some bacterial defense mechanisms specific to HOCl stress—including three transcriptional regulators (HypT, RclR, and NemR) and four chaperone holdases (Hsp33, RidA, Cnox, and polyP)—these provide only limited protection. Critically, these mechanisms don’t prevent HOCl from killing bacteria; they merely help some cells survive sub-lethal exposure. Even bacteria with these defense systems activated remain susceptible to therapeutically relevant HOCl concentrations. Some studies have shown that certain bacteria can adapt to low levels of sodium hypochlorite (bleach) under specific laboratory conditions. However, as noted in 2025 research, such resistance is “infrequent” and has not been observed clinically with properly formulated HOCl solutions used at appropriate concentrations. The Biofilm Advantage One of HOCl’s most significant advantages emerges in the context of biofilms—those bacterial fortresses that render conventional antibiotics largely ineffective. Research published in 2025 demonstrates that stabilized HOCl solutions maintain antimicrobial activity within biofilms at dilutions ranging from 1/32 to 1/16. More impressively, the concentration needed to kill bacteria within biofilms is the same as that needed to prevent biofilm formation—a stark contrast to antibiotics, which typically require 100-1,000 times higher concentrations to achieve biofilm penetration. HOCl achieves this through several mechanisms: Clinical Applications: From Wounds to Respiratory Infections The unique properties of HOCl have led to expanding clinical applications: Wound Care FDA-cleared HOCl solutions are revolutionizing chronic wound management. A 2025 study showed that HOCl’s rapid antimicrobial action combined with wound healing enhancement properties makes it ideal for treating infected wounds without the risk of resistance development. Respiratory Applications Recent research exploring HOCl for respiratory infections shows promising results. As a 2025 article in Viruses notes, HOCl’s successful history in wound treatment, combined with low cytotoxicity and documented efficacy against respiratory pathogens (including influenza and SARS-CoV-2), suggests significant potential for inhalation therapy. Surgical Site Preparation HOCl solutions are increasingly used for pre-operative skin antisepsis. Studies demonstrate significant bacterial load reduction without altering microbial diversity—avoiding the risk of opportunistic infections that can occur with broad-spectrum antibiotics. Environmental Disinfection Healthcare facilities are adopting HOCl for surface disinfection, particularly in areas requiring frequent cleaning where traditional disinfectants pose toxicity concerns or leave harmful residues. The Stability Challenge: Not All HOCl Is Equal Traditional HOCl solutions face a significant limitation: instability. Conventional production methods create HOCl that degrades rapidly (within 90 days) and loses efficacy in the presence of organic matter—precisely the conditions found in clinical use. This limitation has historically prevented HOCl from achieving its full therapeutic potential. However, recent advances in stabilization technology have produced HOCl formulations that: These next-generation HOCl solutions represent a paradigm shift in antimicrobial therapy. Safety Profile: Gentle Yet Powerful One of HOCl’s most remarkable characteristics is its safety profile. Unlike many antimicrobial agents that demonstrate toxicity concerns, HOCl is: Non-Toxic to Human Cells Because HOCl is naturally produced by the body, human cells have evolved mechanisms to handle it. At therapeutic concentrations, HOCl solutions don’t damage healthy tissue. Promotes Wound Healing Research demonstrates that HOCl has dose-dependent favorable effects on fibroblast and keratinocyte migration—the cells responsible for wound closure. This means HOCl doesn’t just kill bacteria; it actively supports healing. No Systemic Absorption When used topically, HOCl doesn’t enter the bloodstream in therapeutically significant amounts, eliminating concerns about systemic toxicity
SPX-001 : Pioneering the Future of Respiratory Infection Treatment
SPX-001 : Pioneering the Future of Respiratory Infection Treatment The Respiratory Infection Challenge Respiratory infections remain among the most significant threats to global health. Hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP) affect thousands of critically ill patients annually, with mortality rates ranging from 20-50% despite aggressive antibiotic therapy. The challenge isn’t just the severity of these infections—it’s the unique environment of the respiratory tract that renders many treatments ineffective. The lungs present a hostile environment for antimicrobial therapy. Thick mucus, abundant blood serum proteins, inflammatory cells, and cellular debris create conditions that dramatically reduce the efficacy of conventional antimicrobials. Traditional hypochlorous acid (HOCl) formulations, despite potent antimicrobial activity in laboratory settings, lose most of their effectiveness when confronted with the complex biochemistry of infected lungs. This is where innovation becomes imperative. Enter SPX-001: a next-generation antimicrobial drug candidate specifically engineered to overcome the limitations that have prevented effective pulmonary infection treatment. SPX-001: Engineering Solutions for Pulmonary Challenges SPX-001 represents a fundamental rethinking of antimicrobial therapy for respiratory infections. Building on proven SPC-069 chemistry, this broad-spectrum antiviral and antibacterial drug candidate addresses the primary factor that limits conventional HOCl efficacy: stability and activity in the presence of serum and biological fluids. The Serum Stability Breakthrough The development team behind SPX-001 identified a critical weakness in traditional antimicrobial approaches: most lose potency when exposed to proteins found in blood and bodily fluids. In infected lungs, where inflammation brings serum proteins into the airway lining fluid, this limitation proves devastating. SPX-001 maintains antimicrobial activity in 5% serum—a concentration that completely inactivates conventional HOCl products. This isn’t a marginal improvement; it’s the difference between therapeutic success and failure in real-world clinical conditions. Mucus Penetration Respiratory infections generate thick, viscous mucus that serves as both a physical barrier and a haven for pathogens. SPX-001’s formulation enables penetration through mucus layers, reaching bacteria and viruses that hide beneath this protective coating. This capability addresses one of the fundamental challenges in treating chronic respiratory infections, particularly in conditions like cystic fibrosis where thick mucus perpetuates infections. The Science Behind SPX-001 Understanding SPX-001’s mechanism reveals why it succeeds where other approaches fail: Broad-Spectrum Activity Unlike narrow-spectrum antibiotics that target specific bacterial classes, SPX-001 demonstrates efficacy against: This broad coverage is particularly valuable in critically ill patients where mixed infections are common and rapid empiric treatment is essential. Rapid Action SPX-001’s antimicrobial effect occurs within minutes, not hours or days. This rapid action prevents bacterial proliferation during the critical early phase of infection when pathogen loads are still manageable and before biofilms can establish. No Resistance Promotion Perhaps most critically, SPX-001’s multi-target mechanism makes resistance development extraordinarily unlikely. As discussed in recent research on HOCl-based therapies, the simultaneous disruption of multiple cellular components—membranes, proteins, nucleic acids—requires bacteria to develop multiple resistance mechanisms simultaneously, an evolutionary near-impossibility. Target Indications: Where SPX-001 Excels Hospital-Acquired Pneumonia (HAP) HAP affects 0.5-2% of hospitalized patients and carries mortality rates of 20-50%. Current treatment relies heavily on broad-spectrum antibiotics, contributing to resistance development. SPX-001 offers an alternative that maintains efficacy against resistant strains while avoiding resistance promotion. Ventilator-Associated Pneumonia (VAP) VAP develops in 9-27% of mechanically ventilated patients, typically caused by bacteria that colonize the oropharynx and are aspirated into the lungs. The presence of endotracheal tubes and breathing circuits creates biofilm-prone surfaces, and accumulated secretions provide ideal conditions for infection. SPX-001’s ability to penetrate mucus, maintain activity in serum, and disrupt biofilms positions it as an ideal candidate for VAP prevention and treatment delivered directly through ventilator circuits. Chronic Respiratory Infections Patients with chronic lung diseases like cystic fibrosis, bronchiectasis, or chronic obstructive pulmonary disease (COPD) experience repeated respiratory infections that progressively damage lung tissue. The biofilm-forming capabilities of pathogens like Pseudomonas aeruginosa make these infections particularly difficult to eradicate. Delivery Method: Direct to the Lungs SPX-001 is designed for inhalation delivery, allowing direct application to infection sites. This approach offers several advantages: Targeted Therapy Delivering antimicrobials directly to the lungs achieves high local concentrations at infection sites while minimizing systemic exposure. This targeted approach reduces potential side effects and drug interactions. Bypassing Serum Limitations While systemic antibiotics must penetrate from the bloodstream through lung tissue into airways (with significant loss of activity along the way), inhaled SPX-001 delivers therapeutic concentrations directly where needed. Rapid Response Inhalation allows immediate contact with pathogens, initiating antimicrobial action within minutes rather than waiting for systemic absorption and distribution. Patient Convenience Nebulizer or inhaler delivery is familiar to respiratory patients and can be administered in hospital or potentially home settings, improving treatment accessibility. The Development Journey Preclinical Optimization Current development focuses on refining formulation parameters: Preclinical studies evaluate: Strategic Partnership: SpectrumX Recognition of SPX-001’s potential led to a significant development milestone: licensing to SpectrumX for UK and European markets. This partnership: The Regulatory Pathway Forward SPX-001’s development follows established regulatory frameworks for new antimicrobial drug approval: Investigational New Drug (IND) Application This critical step enables human clinical trials, requiring comprehensive preclinical data on: Phase 1 Clinical Trials Initial human studies will evaluate: Phase 2 Clinical Trials Proof-of-concept studies in patients with respiratory infections will assess: Phase 3 Clinical Trials Large-scale trials will provide: The Unmet Need SPX-001 Addresses Current respiratory infection treatment faces multiple challenges: Antibiotic Resistance Increasing rates of multidrug-resistant respiratory pathogens limit treatment options. When first-line antibiotics fail, clinicians must resort to toxic second-line agents with significant side effects. Treatment Failures Even with appropriate antibiotic selection, penetration into infected lung tissue often proves inadequate. Biofilms, mucus plugging, and serum protein binding reduce efficacy. Limited Viral Options While bacterial pneumonias have multiple antibiotic options (albeit increasingly resistant), viral respiratory infections have few targeted treatments. SPX-001’s antiviral activity addresses this gap. Safety Concerns Systemic antibiotics carry risks of organ toxicity, drug interactions, and disruption of normal microbiota. Topical pulmonary delivery of SPX-001 minimizes these concerns. Competitive Advantages SPX-001 distinguishes itself from existing and emerging respiratory antimicrobials: Versus Conventional Antibiotics: Versus Other Topical Antimicrobials: Versus Antiseptic Inhalations: Looking Ahead: The Clinical Future Success of SPX-001 in clinical development
From Lab to Clinic – The Regulatory Journey of Medical Device Innovation
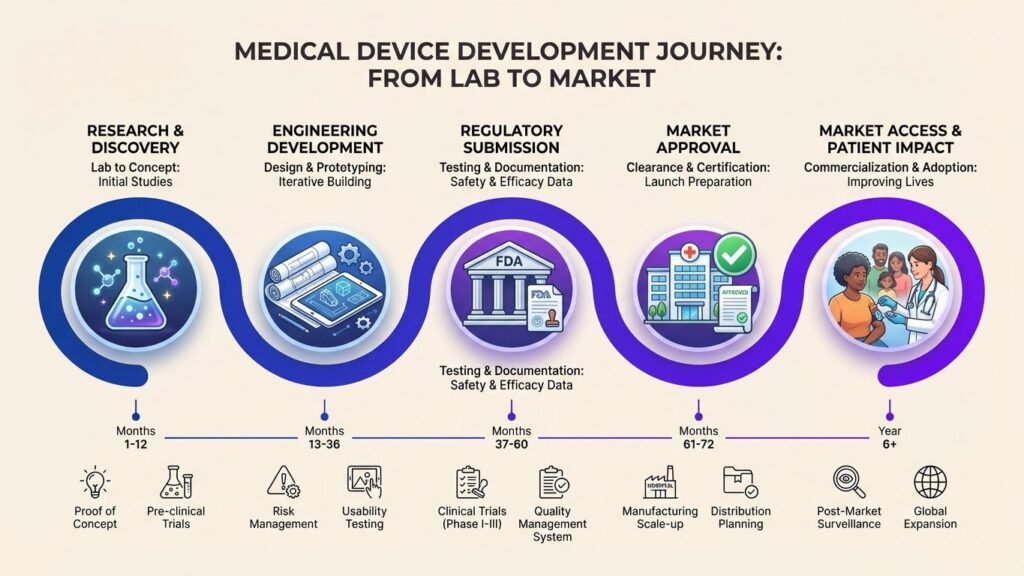
From Lab to Clinic : The Regulatory Journey of Medical Device Innovation The Innovation Paradox A breakthrough medical device sits in a laboratory. Clinical data suggests it could transform patient care. Engineers have perfected the design. Manufacturing processes are robust. Yet it remains years away from helping patients. Why? The answer lies in a complex regulatory framework designed to ensure that medical devices reaching patients are safe, effective, and manufactured to consistent quality standards. While this process can seem daunting—particularly for innovative startups and academic researchers—understanding the regulatory pathway is essential for successfully bringing medical innovations to market. In 2025, the FDA continues to balance two critical mandates: protecting public health through rigorous review while facilitating timely access to innovations that address unmet medical needs. For companies developing next-generation antimicrobial devices and therapies, navigating this landscape requires strategic planning, quality-focused execution, and often, patience. Understanding Device Classification: The Foundation The FDA’s regulatory requirements for medical devices are risk-based. Every medical device falls into one of three classes, determining the level of regulatory control required: Class I Devices: Lowest Risk These devices pose minimal risk to users. Examples include elastic bandages, examination gloves, and hand-held surgical instruments. Most Class I devices are exempt from premarket review, requiring only registration and listing with the FDA. Class II Devices: Moderate Risk These devices require greater regulatory control to ensure safety and effectiveness. Most antimicrobial wound care products fall into this category. Class II devices typically require 510(k) premarket notification demonstrating “substantial equivalence” to a legally marketed device. Class III Devices: Highest Risk These devices support or sustain human life, are implanted, or present significant risk of illness or injury. Examples include heart valves, implantable pacemakers, and some high-risk drug-device combinations. Class III devices require premarket approval (PMA), the most stringent regulatory pathway. Understanding your device’s classification is the critical first decision point that impacts development strategy, timeline, and costs. The 510(k) Pathway: Demonstrating Substantial Equivalence For many antimicrobial medical devices, the 510(k) pathway represents the most efficient route to market. Under the Medical Device User Fee Amendments (MDUFA) V, the FDA aims to clear 95% of 510(k) submissions within 90 FDA days. What is Substantial Equivalence? A device is substantially equivalent to a predicate device if it: Building a Strong 510(k) Submission Success in the 510(k) pathway requires: Common 510(k) Pitfalls to Avoid As noted in 2025 regulatory guidance, frequent issues include: The PMA Pathway: When Innovation Requires More For truly novel devices or those presenting significant risk, the PMA pathway provides a mechanism for FDA approval based on scientific evidence that the device is safe and effective for its intended use. PMA Requirements A PMA application includes: PMA Timeline Under current FDA performance goals, PMA average total time to decision approximates 285 days, though complex devices may require longer review periods. The Critical Role of Quality Systems Regardless of regulatory pathway, robust quality management systems (QMS) form the foundation of successful device development. The FDA’s Quality System Regulation (21 CFR Part 820) requires manufacturers to have comprehensive systems covering: Design Controls Manufacturing Controls Documentation and Record Keeping Building quality systems early—during development, not after—dramatically increases regulatory success rates and reduces costly remediation later. The Power of Pre-Submission: Q-Submissions One of the most valuable yet underutilized tools for device developers is the FDA’s Q-Submission program. This mechanism allows companies to obtain FDA feedback before formal submission. Q-Submission Types Include: According to 2025 regulatory data, companies using pre-submissions strategically achieve significantly higher first-pass approval rates and shorter review times. Timing is Critical Engage FDA early—ideally when you’ve characterized your device and planned initial testing but before generating all data. This timing allows incorporation of FDA feedback without costly redoing of studies. Accelerated Pathways: Breakthrough Devices Program For devices offering significant advantages over existing treatments for life-threatening or irreversibly debilitating conditions, the FDA’s Breakthrough Devices Program provides expedited development and review. Program Benefits Include: Recent analysis shows Breakthrough designation can reduce time to market by 6-12 months for qualifying devices. The Global Perspective: CE Mark and Beyond While FDA approval enables U.S. market access, global commercialization requires navigating additional regulatory frameworks: European Union: CE Mark Under the Medical Device Regulation (MDR), devices must: Other Key Markets Strategic regulatory planning addresses multiple markets simultaneously, maximizing return on development investment. The Post-Market Reality: Obligations Don’t End at Approval FDA approval or clearance marks the beginning, not the end, of regulatory obligations: Post-Market Surveillance Quality System Inspections FDA conducts inspections of device manufacturers to verify QMS compliance. Preparation for inspections should be continuous, not triggered by inspection announcement. Post-Market Studies In some cases, FDA requires post-approval studies to gather additional real-world evidence about device performance, particularly for novel technologies or those approved through accelerated pathways. Real-World Example: Our Journey Our experience developing FDA-cleared antimicrobial wound care devices illustrates these principles in practice: Phase 1: Foundation Building (Year 1) Phase 2: Regulatory Preparation (Year 2) Phase 3: FDA Review and Approval (Year 2-3) Phase 4: International Expansion (Year 3-4) This journey required significant investment, careful planning, and unwavering commitment to quality—but resulted in cleared medical devices now benefiting patients globally. Lessons Learned: Success Factors Through this experience, several success factors emerged: 1. Quality from Day One Building quality systems early prevents costly remediation and delays. Quality isn’t something added at the end; it’s fundamental from the beginning. 2. FDA Engagement Viewing FDA as a partner, not adversary, through early engagement and transparent communication dramatically improves outcomes. 3. Scientific Rigor Robust testing and clear documentation of results builds FDA confidence and accelerates review. 4. Expert Guidance Engaging regulatory consultants with device-specific expertise helps navigate complex requirements and avoid common pitfalls. 5. Resource Planning Regulatory processes require significant resources—human, financial, and time. Realistic planning prevents mid-process resource crises. The Cost of Innovation: Investment Required Regulatory compliance and clinical development require substantial investment: Typical 510(k) Program Costs: PMA Program Costs: Post-Market Costs: These figures underscore why many academic innovations fail to reach commercialization—the “valley of death” between proof of concept and